¶ Overview
- McGuire voted for a bill that would kick 17 million Americans off their health insurance, including nearly 12 million Americans off of Medicaid. More than 35,000 Virginians in his district could lose their health coverage as a result of his votes. Nine rural health clinics across Virginia were at risk of closing or significantly reducing services due to the Medicaid cuts, and Augusta Medical Group closed three clinics in anticipation of the Republican Bill’s impact on their operations.
¶ McGuire Voted To Kick More Than 35,000 Of His Constituents And Nearly 12 Million Americans Off Medicaid
¶ McGuire Voted Three Times to take health coverage from Virginians
¶ July 2025: McGuire Voted For The Final Version Of Republicans’ Reconciliation Bill
7/3/25: McGuire Voted For The Senate FY 2025 Budget Reconciliation Bill That Cut Medicaid And Other Social Programs To Offset The Bill’s Costs. In July 2025, McGuire voted for, according to Congressional Quarterly, the “motion to concur in the Senate amendment to the bill that would permanently extend nearly $4 trillion in expiring individual and business tax cuts, create several new tax breaks and fund border and immigration enforcement and air traffic control upgrades. It would cut Medicaid and other safety net programs to partly offset the cost. Among other provisions, it would raise the statutory debt ceiling by $5 trillion and appropriate more than $448 billion in mandatory funding for Trump administration priorities and other needs, including $153 billion for defense, $89 billion for immigration enforcement, and $89.5 billion for border control and security. It also would increase the state and local tax deduction cap to $40,000 annually for five years for households making up to $500,000 a year until 2030, when it would permanently revert to $10,000.” The House passed the bill by a vote of 218 to 214. [House Vote 190, 7/3/25; Congressional Quarterly, 7/3/25; Congressional Actions, H.R. 1]
- HEADLINE: "At Least 17 Million Americans Would Lose Insurance Under Trump Plan" [Washington Post, 7/1/25]
- The Congressional Budget Office Estimated That 11.8 Million People Would Become Uninsured As A Result Of The Medicaid Cuts In Republicans’ Reconciliation Bill. According to the Washington Post, "The bill, which narrowly passed the Senate on Tuesday and now heads back to the House, would effectively accomplish what Republicans have long failed to do: unwind many of the key components of the ACA, President Barack Obama’s signature domestic achievement, which dramatically increased the number of Americans with access to health insurance. To start, the Congressional Budget Office estimated that the Senate version of the bill would result in 11.8 million more uninsured in 2034, mostly because of Medicaid cuts, compared with 10.9 million if the House version became law." [Washington Post, 7/1/25]
¶ May 2025: McGuire Voted For House Republicans’ Budget Bill, Which Would Kick Millions Of People Off Medicaid
5/22/25: McGuire Voted For The FY 2025 Budget Reconciliation Bill That Included $3.8 Trillion In Tax Cuts Offset By $1.5 Trillion In Spending Reductions To Programs Like Medicaid And The Supplemental Nutrition Assistance Program. In May 2025, McGuire voted for, according to Congressional Quarterly, “the bill that would provide for approximately $3.8 trillion in net tax cuts and $321 billion in military, border enforcement and judiciary spending, offset by $1.5 trillion in spending reductions, as instructed in the fiscal 2025 budget resolution (H Con Res 14). It would raise the statutory debt limit by $4 trillion and provide for increased spending on defense and border security, spending cuts on social safety net programs, such as Medicaid and the Supplemental Nutrition Assistance Program. It also includes a mix of tax breaks for businesses and individuals; tax increases on universities and foundations; and a phase-down of clean energy tax credits. […] It would reduce federal spending on the Supplemental Nutrition Assistance Program by requiring states to shoulder more of the cost, expand work requirements for SNAP, extend programs authorized under the 2018 farm bill, and prohibit the U.S. Department of Agriculture from increasing the cost of the Thrifty Food Program. As amended, it would cap state and local tax deductions at $40,000 for households with incomes below $500,000.” The House passed the bill by a vote of 215 to 214. [House Vote 145, 5/22/25; Congressional Quarterly, 5/22/25; Congressional Actions, H.R. 1]
- The House GOP Budget Bill Was Estimated To Increase The Uninsured Population By 8.6 Million By 2034. According to CNN, “The Medicaid and Affordable Care Act provisions in the package could result in 8.6 million more people being uninsured in 2034, according to an early CBO estimate released by Democratic lawmakers. That number is expected to grow with the latest changes.” [CNN, 5/28/25]
- The House GOP Budget Bill Codified A Trump Administration Proposal That Restricted Access To The Affordable Care Act. According to CNN, “The bill also calls for codifying a Trump administration proposal that would make changes to the Affordable Care Act enrollment process, including shortening the open enrollment period and eliminating the ability of low-income Americans to sign up year-round.” [CNN, 5/28/25]
¶ February 2025: McGuire Voted For A Budget Resolution That Spelled Out Future Medicaid Cuts
2/25/25: McGuire Voted For The FY 2025 Budget Framework That Included $2 Trillion In Cuts, Raised The Statutory Debt Limit By $4 Trillion, And Required House Committees To Recommend Legislation That Would Implement Trump’s Agenda. In February 2025, McGuire voted for, according to Congressional Quarterly, “the concurrent resolution that would recommend a budget for fiscal 2025 and budget levels through fiscal 2034. The resolution would assume minimum savings of $1.5 trillion over 10 years and 2.6 percent economic growth over the same period. It also would require the statutory debt limit to be raised by $4 trillion. It also would authorize the House Ways and Means Committee to increase deficits by $4.5 trillion over 10 years to extend the 2017 tax cuts and implement new tax cuts proposed by the White House. It also would provide instructions for the budget reconciliation process through which separate legislation could be considered and passed in the Senate via a simple majority vote. The measure would deliver instructions to 11 House committees to report legislation that would implement President Donald Trump’s agenda, such as expanding tax cuts and bolstering border security and immigration enforcement. The committees would be required to report their legislative recommendations to the House Budget Committee by March 27, 2025. It also would set a $2 trillion target for the spending cuts to be submitted to the House Budget Committee. The resolution also would stipulate that if the committees don't reach that target, the Ways and Means’ reconciliation instructions to increase the deficit by a maximum of $4.5 trillion would be decreased by the amount the other committees come in below the target. Similarly, it would stipulate that Ways and Means could increase the deficit above the $4.5 trillion level by the amount of savings the committees achieve above the $2 trillion target.” The vote was on passage. The House passed the resolution by a vote of 217 to 215. [House Vote 50, 2/25/25; Congressional Quarterly, 2/25/25; Congressional Actions, H. Con. Res. 14]
- HEADLINE: “What Can House Republicans Cut Instead Of Medicaid? Not Much.” [New York Times, 2/25/25]
- HEADLINE: "House Republican Budget Takes Away Health Care, Food Aid To Pay For Expanded Tax Cuts For Wealthy" [Center on Budget and Policy Priorities, 2/21/25]
- New York Times Reported The $880 Billion In Cuts Required By The Republican Budget Proposal Would Have To Come From Medicaid, Medicare, Or CHIP. According to the New York Times, "The budget resolution itself is silent on whether Congress cuts Medicaid, which provides health coverage to 72 million poor and disabled Americans. But it instructs the House Energy and Commerce Committee, which has jurisdiction over the program, to cut spending by $880 billion over the next decade. If the committee can’t save at least that much, the entire effort could be imperiled because of the special process Congress is using to avoid a Senate filibuster. Ten other committees have their own instructions to follow, though none have been assigned with cutting nearly as much. It’s not so simple as finding the cuts elsewhere. The special process, known as budget reconciliation, means Republicans will have to find all $880 billion from within the Energy and Commerce Committee’s jurisdiction. That leaves them with fewer options than one might think. […] If Republicans want to avoid major cuts to Medicaid, the largest pot of available money is in the other big government health insurance program: Medicare. […] Even if the committee cuts everything that’s not health care to $0, it will still be more than $600 billion short. The committee could also save around $200 billion by eliminating the Children’s Health Insurance Program, but that option has not been raised by the budget committee or anyone in House leadership. […] Even if all of these cuts, revenues and rule cancellations from outside health care can pass muster, the committee will still be left with hundreds of billions of dollars to cut to hit its goal. Mathematically, the budget committee’s instructions mean the committee would need to make major cuts to either Medicare, Medicaid or both." [New York Times, 2/25/25]
¶ McGuire touted passage of the big BEAUTIFUL bill and claimed republicans delivered for the american people
July 2025: McGuire Praised The Passage Of The Republican Budget Bill And Claimed Republicans “Delivered For The American People” By Passing The Legislation. According to a press release from Rep. John McGuire, “U.S. Representative John McGuire (VA-05), voted for the Senate Amendment to H.R. 1, the One Big Beautiful Bill Act. The One Big Beautiful Bill Act advances President Trump’s America First agenda, prevents the largest tax hike in American history, provides for American energy dominance, secures our border, supports families and small businesses, and cuts wasteful spending. ‘Promises Made, Promises Kept. Congressional Republicans and President Trump delivered for the American people by passing the One Big Beautiful Bill,’ said Rep. John McGuire. ‘The One Big Beautiful Bill Act prevents the largest tax increase on middle- and working-class Americans in our nation’s history. This legislation includes no tax on tips, no tax on overtime, and a tax deduction for seniors. This allows American families to save more of the money they earned. Additionally, this legislation includes historic spending reforms that secure over $1 trillion in savings, secures our border, and provides for American energy dominance. The One Big Beautiful Bill truly invests in American workers, businesses, and families. Thank you to President Trump for putting America First.’” [Press Release – Rep. John McGuire, 7/9/25]
¶ More Than 35,000 Virginians In The Fifth Congressional District Could Lose Health Coverage A Result Of McGuire’s Votes
An Estimated 35,963 People In McGuire’s District On The Affordable Care Act And Medicaid Were Set To Lose Coverage Due To Republican Budget Bill Health Care Cuts. According to the Joint Economic Committee,

[Joint Economic Committee, Viewed 10/17/25]
2023: 162,000 Virginians In The 5th Congressional District Were Enrolled In Medicaid Or CHIP. According to the Center for American Progress,

[Center for American Progress, 3/11/25]
¶ McGuire’s votes for the big beautiful bill created problems for virginia hospitals
HEADLINE: “Virginia Hospitals Could Lose Up To $26B Due To Federal Medicaid Cuts” [VPM News, 7/22/25]
- The Republican Budget Bill’s Changes To Managed Care Organizations Were Estimated To Cost Virginia $26 Billion Over 14 Years. According to VPM News, “The new federal law — legislation once known as the ‘One Big Beautiful Bill’ that Trump signed on July 4 — is expected to slash federal funding for Medicaid, the government-backed program providing health care coverage for eligible low-income adults, families, children, pregnant people and people with disabilities. It will bring new requirements for Medicaid members and restrictions on taxes levied on hospitals. The nonpartisan Congressional Budget Office estimates it will lead to 10 million fewer people with health insurance in 2034. In Medicaid expansion states like Virginia, the law also calls for Medicaid managed care organizations to reduce payments to health care providers by 10% each year starting in 2028 until it’s 100% of the Medicare rate. This change to state-directed payments is estimated to cause a $26 billion reduction over 14 years because MCOs in Virginia pay providers well over the Medicare rate, according to Chris Gordon, the chief financial officer of Virginia’s Department of Medical Assistance Services.” [VPM News, 7/22/25]
- The Chief Financial Officer Of Virginia’s Department Of Medical Assistance Services Said The Republican Budget Bill Would Cause A “Macroeconomic Financial Shock” Across The State. According to VPM News, “Gordon told lawmakers last week that modeling shows such a loss in funding would have significant ramifications for the state’s economy. The cuts will create ‘a macroeconomic financial shock, not just to the hospitals, but also for the state writ large,’ Gordon told the General Assembly’s Joint Subcommittee for Health and Human Resources Oversight in a presentation on July 15. Gordon added: ‘There will be a reduction in labor force participation — because the quickest thing to do is reduce head counts when you're faced with something like that — as well as population, as people move to try and migrate out to do jobs elsewhere.’” [PBS VPM, 7/22/25]
The Virginia Hospital And Healthcare Association Estimated $2 Billion In Annual Medicaid Cuts Due To The Republican Budget Bill. According to Axios, “Virginia hospitals and free clinics were already bracing for a Medicaid overhaul, part of President Trump's tax and spending bill, which could strip coverage from nearly 600,000 residents by 2027. State hospitals face $2 billion in annual Medicaid cuts once changes go into full effect in October 2027, Virginia Hospital & Healthcare Association spokesperson Julian Walker told Axios. Walker noted that the uncertainty is happening as hospitals continue to recover financially from the COVID pandemic.” [Axios, 10/6/25]
- According To The Center For Healthcare Quality And Payment Reform, Nearly A Third Of Virginia’s Rural Hospitals Were At Risk Of Closing In August 2025. According to Axios, “Nearly a third of Virginia's rural hospitals (9) were at risk of closing in August, per the Center for Healthcare Quality & Payment Reform. And last month, Augusta Medical Group announced it had closed three urgent and primary care clinics in southwest Virginia ahead of Medicaid changes. Between the lines: Closures or cutbacks could mean job losses, longer commutes for care and a strain on free clinics, which have said they lack the resources to absorb the surge of uninsured patients if people lose coverage.” [Axios, 10/6/25]
September 2025: Augusta Medical Group Closed Three Clinics And Cited The Republican Budget Bill As The Reason For Closing Them. According to the Virginia Mercury, “Augusta Medical Group is closing an urgent care clinic and two primary care clinics in response to the massive reconciliation bill Congress passed this summer. The move will force Shenandoah Valley residents to travel further for their primary and emergency health care needs. Dubbed the One Big Beautiful Bill Act, the federal legislation entails forthcoming changes to Medicaid that’s projected to lead to enrollment drop offs and big tweaks to hospital funding mechanisms. First reported by WHSV3, and according to a press release from Augusta Medical Group, Augusta Medical Group’s decision is part of the ‘ongoing response’ to the OBBA and ‘the resulting realities for healthcare delivery.’” [Virginia Mercury, 9/8/25]
¶ June 2026: A Report PUBLISHED BY The Virginia Joint Commission On Health Care Found That Two Rural Hospitals In McGuire’s District Were At Risk Of Closing
¶ A Report From The Virginia Joint Commission On Health Care Found One Rural Hospital In McGuire’s District Was At An “Immediate Risk Of Closure” And Another Was “At Risk Of Closure”
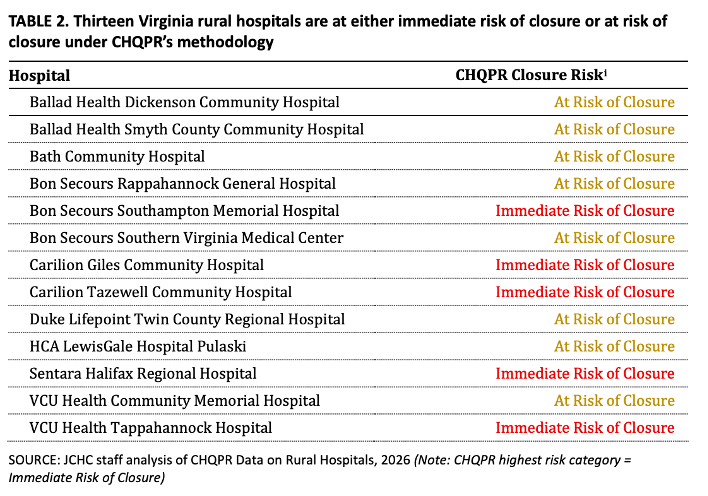
Sentara Halifax Regional Hospital In South Boston, VA Was Deemed At An “Immediate Risk Of Closure” By The Joint Commission On Health Care. According to a report published by the VA Joint Commission on Health Care, “CHQPR’s findings indicate that a significant proportion of rural hospitals in the United States are operating with negative patient service margins, and many also have limited or declining reserves. In 2026, the CHQPR analysis estimates that 309 rural hospitals nationwide fall into the immediate risk of closure category while 734 fall into the at risk of closure category (see APPENDIX 2 for full CHQPR risk categories by state). CHQPR classifies five rural hospitals in Virginia as being at immediate risk of closure and eight as at highest risk of closure (TABLE 2)”
[VA Joint Commission on Health Care, Page 12, Viewed 6/11/26]
- The Commission Relied On Methodology Created By CHQPR, Which Analyzed Indicators Of Rural Hospital Financial Performance To Identify Hospitals At Risk Of Closure. According to a report published by the VA Joint Commission on Health Care, “The Center for Healthcare Quality and Payment Reform (CHQPR) analyzes indicators of rural hospital financial performance to identify rural hospitals throughout the country that are at high risk of closure due to financial conditions. The Financial Distress Index (FDI), developed by the Cecil G. Sheps Center for Health Services Research at the University of North Carolina, combines analysis of financial performance with evaluation of operational and market-level factors that may influence financial performance to identify rural hospitals at high risk of financial distress and instability. These models can be used in tandem to identify rural hospitals in Virginia at highest risk of experiencing financial distress or closure.” [VA Joint Commission on Health Care, Page 11, Viewed 6/11/26]
- Under CHQPR’s Methodology, A Rural Hospital Was At “Immediate Risk Of Closure” If It Had Negative Patient Service Operating Margins And Low Or Negative Net Assets. According to a report published by the VA Joint Commission on Health Care, “Hospitals with negative patient service operating margins and low or negative net assets are categorized as being at immediate risk of closure, as they are both operating at a loss and lack sufficient reserves to offset those losses. Hospitals that have either negative patient service operating margins or low or negative net assets are categorized as at risk of closure. Data on hospital financial performance are derived directly from financial information reported by each facility and reflect a point-in-time assessment of each facility's financial viability.” [VA Joint Commission on Health Care, Page 11, Viewed 6/11/26]
VCU Health Community Memorial Hospital In South Hill, VA Was Deemed “At Risk Of Closure” By The Joint Commission On Health Care. According to a report published by the VA Joint Commission on Health Care, “CHQPR’s findings indicate that a significant proportion of rural hospitals in the United States are operating with negative patient service margins, and many also have limited or declining reserves. In 2026, the CHQPR analysis estimates that 309 rural hospitals nationwide fall into the immediate risk of closure category while 734 fall into the at risk of closure category (see APPENDIX 2 for full CHQPR risk categories by state). CHQPR classifies five rural hospitals in Virginia as being at immediate risk of closure and eight as at highest risk of closure (TABLE 2)”
[VA Joint Commission on Health Care, Page 12, Viewed 6/11/26]
- The Commission Relied On Methodology Created By CHQPR, Which Analyzed Indicators Of Rural Hospital Financial Performance To Identify Hospitals At Risk Of Closure. According to a report published by the VA Joint Commission on Health Care, “The Center for Healthcare Quality and Payment Reform (CHQPR) analyzes indicators of rural hospital financial performance to identify rural hospitals throughout the country that are at high risk of closure due to financial conditions. The Financial Distress Index (FDI), developed by the Cecil G. Sheps Center for Health Services Research at the University of North Carolina, combines analysis of financial performance with evaluation of operational and market-level factors that may influence financial performance to identify rural hospitals at high risk of financial distress and instability. These models can be used in tandem to identify rural hospitals in Virginia at highest risk of experiencing financial distress or closure.” [VA Joint Commission on Health Care, Page 11, Viewed 6/11/26]
- Under CHQPR’s Methodology, A Rural Hospital Was “At Risk Of Closure” If It Had Either Negative Patient Service Operating Margins Or Low Or Negative Net Assets. According to a report published by the VA Joint Commission on Health Care, “Hospitals with negative patient service operating margins and low or negative net assets are categorized as being at immediate risk of closure, as they are both operating at a loss and lack sufficient reserves to offset those losses. Hospitals that have either negative patient service operating margins or low or negative net assets are categorized as at risk of closure. Data on hospital financial performance are derived directly from financial information reported by each facility and reflect a point-in-time assessment of each facility's financial viability.” [VA Joint Commission on Health Care, Page 11, Viewed 6/11/26]
¶ A Report From The Virginia Joint Commission On Health Care Found One Rural Hospital In McGuire’s District Was At Highest Risk Of Experiencing Financial Distress And Another Was At Mid-Risk Of Experiencing Financial Distress
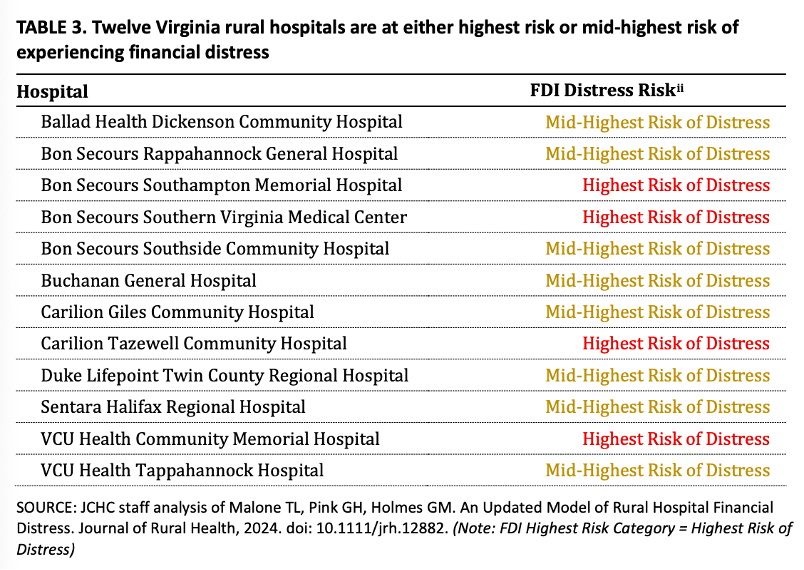
VCU Health Community Memorial Hospital Was Deemed At “Highest Risk Of Distress” By The Joint Commission On Health Care. According to a report published by the VA Joint Commission on Health Care, “The 2025 FDI prediction, the most current available, identifies 86 hospitals as meeting the criteria for highest risk of experiencing distress and 329 hospitals as meeting the criteria for mid-highest risk of experiencing distress (see APPENDIX 3 for full FDI risk categories by state). In Virginia, four hospitals meet FDI's criteria for highest risk of experiencing distress and eight meet the criteria for mid-highest risk of experiencing distress (TABLE 3).”
[VA Joint Commission on Health Care, Page 13-14, Viewed 6/11/26]
- The Commission Relied On The UNC Sheps Center’s Financial Distress Index (FDI), Which Measured Market-Level Factors And A Rural Hospital’s Financial Performance And Organizational Characteristics To Make Its Determinations. According to a report published by the VA Joint Commission on Health Care, “The FDI model incorporates several categories of inputs to determine rural hospital financial condition and identify rural hospitals that may be at risk of financial instability. Financial performance measures, such as operating margin, liquidity, and net assets, indicate whether a hospital's core patient care activities generate sufficient revenue to cover expenses and the hospital's ability to meet short-term financial obligations and continue operating without disruption. Analysis of organizational characteristics, such as hospital size and ownership type, provide insight into hospitals' access to capital, administrative capacity, and sources of financial support. Market-level factors, including local income levels, payer mix, and population characteristics, reflect the external environment in which the hospital operates and influence both demand for services and reimbursement levels that drive revenue.” [VA Joint Commission on Health Care, Page 13, Viewed 6/11/26]
Sentara Halifax Regional Hospital Was Deemed At “Mid-Highest Risk Of Distress” By The Joint Commission On Health Care. According to a report published by the VA Joint Commission on Health Care, “The 2025 FDI prediction, the most current available, identifies 86 hospitals as meeting the criteria for highest risk of experiencing distress and 329 hospitals as meeting the criteria for mid-highest risk of experiencing distress (see APPENDIX 3 for full FDI risk categories by state). In Virginia, four hospitals meet FDI's criteria for highest risk of experiencing distress and eight meet the criteria for mid-highest risk of experiencing distress (TABLE 3).”
[VA Joint Commission on Health Care, Page 13-14, Viewed 6/11/26]
- The Commission Relied On The UNC Sheps Center’s Financial Distress Index (FDI), Which Measured Market-Level Factors And A Rural Hospital’s Financial Performance And Organizational Characteristics To Make Its Determinations. According to a report published by the VA Joint Commission on Health Care, “The FDI model incorporates several categories of inputs to determine rural hospital financial condition and identify rural hospitals that may be at risk of financial instability. Financial performance measures, such as operating margin, liquidity, and net assets, indicate whether a hospital's core patient care activities generate sufficient revenue to cover expenses and the hospital's ability to meet short-term financial obligations and continue operating without disruption. Analysis of organizational characteristics, such as hospital size and ownership type, provide insight into hospitals' access to capital, administrative capacity, and sources of financial support. Market-level factors, including local income levels, payer mix, and population characteristics, reflect the external environment in which the hospital operates and influence both demand for services and reimbursement levels that drive revenue.” [VA Joint Commission on Health Care, Page 13, Viewed 6/11/26]
¶ Sentara Halifax Regional Hospital And VCU Health Community Memorial Hospital In McGuire’s District Were Two Of Virginia’s Most Financially Vulnerable Rural Hospitals
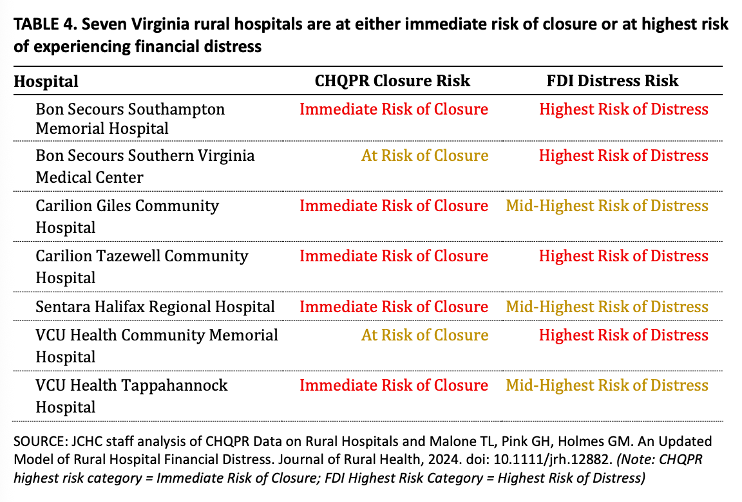
The Commission Determined That Sentara Halifax Regional Hospital And VCU Health Community Memorial Hospital Were Two Of The Seven Most Financially Vulnerable Rural Virginia Hospitals. According to a report published by the VA Joint Commission on Health Care, “Taken together, the CHQPR framework and the UNC Sheps Center FDI model identify a subset of rural hospitals in Virginia that are at the highest risk of financial distress or closure. Of Virginia's 36 rural hospitals, two are identified in the highest categories of both models - as at immediate risk of closure by the CHQPR framework and as at highest risk of experiencing distress by the FDI model. An additional three are identified as at immediate risk of closure by the CHQPR framework while meeting criteria for being at mid-highest risk of experiencing distress by the FDI model. The final two are identified as at risk of closure by the CHQPR framework and as meeting criteria for highest risk of distress by the FDI model (TABLE 4). Altogether, seven rural hospitals meet criteria for the highest risk category as measured by at least one of these models.”
[VA Joint Commission on Health Care, Page 15-16, Viewed 6/11/26]